CAR-T’s clinical and manufacturing considerations highlight the importance of earlier treatment in relapsed or refractory multiple myeloma (RRMM).
Attrition Rates
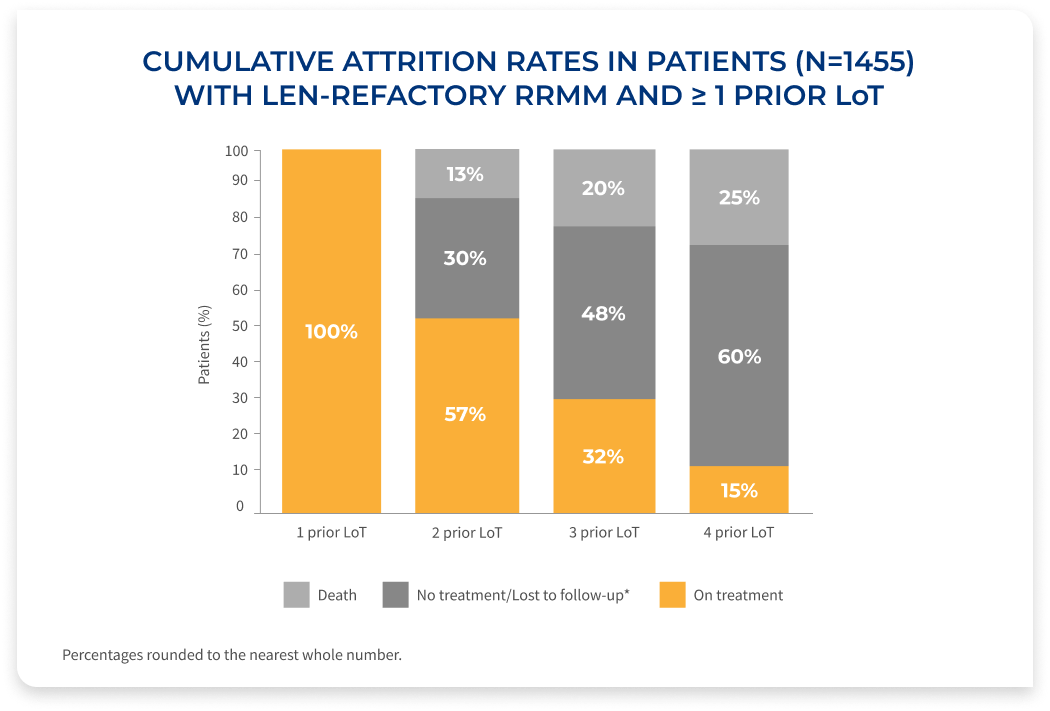
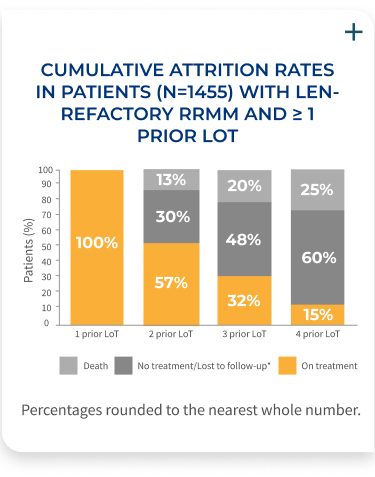
Fewer patients make it to the next line of therapy1
The percentage of patients on treatment decreases with each LoT, demonstrating the need for efficacious therapies at first relapse in RRMM.
Results of a retrospective database analysis (January 2016-April 2022) of 1,455 RRMM patients with 1-3 prior LoT, ECOG PS <2, who were exposed to PI and an immunomodulatory agent, and were considered len-refractory.
Study overview
- Patients had an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of <2 and were derived from the Flatiron Health de-identified US electronic health records database (January 2016–April 2022)
- Patients who are len-refractory were defined as having a change in treatment within 60 days of last lenalidomide therapy without lenalidomide as a component of the immediate next LoT. Index date was defined as the start of first therapy (index therapy) after a patient met the inclusion criteria
- Daratumumab/pomalidomide/
dexamethasone (DPd) was the most commonly used index regimen (13.2%), followed by daratumumab monotherapy (8.3%), Pd (7.7%), carfilzomib/
pomalidomide/dexamethasone (KPd) (7.1%), and Kd (7.0%)
CAR-T=chimeric antigen receptor-T cell; len=lenalidomide; LoT=line(s) of therapy; PI=proteasome inhibitor.
*Patients who received an active antimyeloma treatment and had ≥1 follow-up assessment but were subsequently lost to follow-up.
T-cell fitness may enhance CAR-T outcomes1-4

T-cell fitness* is greater earlier in the disease course and may be associated with improved outcomes1-4
- T-cell exhaustion has been attributed to prior treatment exposures, such as alkylating therapies (eg, bendamustine) and underlying MM2-5
- CAR-T cells derived from T-cells earlier in the disease course may be associated with improved outcomes (manufacturing, cell expansion, and cytotoxicity)2,4
Bridging therapy may help reduce AEs of CAR-T therapy6,7

Bridging therapy (BT) is a plasma cell-directed therapy administered during the manufacturing period6
- The time required for CAR-T manufacturing may allow tumor progression that can impact the safety of CAR-T cell infusion6
- The goal of BT is to avoid clinical deterioration and reduce disease burden after apheresis6
- BT is a recommended strategy to control disease and reduce tumor burden during CAR-T cell manufacturing, particularly in patients with aggressive or high-burden disease6
- Patients with a high disease burden or rapidly progressing disease prior to CAR-T infusion have an increased risk for more severe CRS and neurotoxicities6
- Prior to CAR-T infusion, BT helps reduce the risk of CRS, ICANS, and prolonged cytopenias7
- Selecting a regimen that does not involve agents to which a patient’s disease has become refractory should be a priority6
Early referral for CAR-T cell therapy facilitates the collection of fitter T-cells and expands the treatment options for bridging therapy1,5
AE=adverse event; CAR-T=chimeric antigen receptor-T cell; CRS=cytokine release syndrome; ICANS-immune effector cell-associated neurotoxicity syndrome; MM=multiple myeloma.
*Based on prior treatment exposure, disease progression, and markers typically associated with T-cell fitness determined by flow cytometry.1,2,4